

- Details
- Written by Super User
- Category: Uncategorised
- Hits: 24695
| PROFILES |
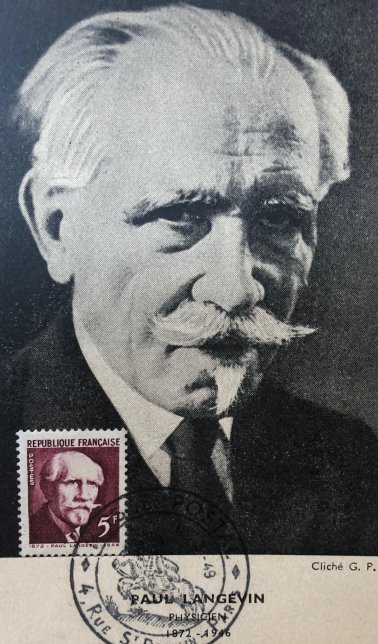
| PAUL LANGEVIN (1872-1946) |
23 January 2022 marks the 150th anniversary of the birth of Paul Langevin, the eminent French physicist who is the father of pulse-echo ultrasound. During 1917, working with the French and British Navies, he designed the first piezoelectric ultrasonic transducers using X-cut quartz. These were operated in pulse-echo mode to detect submarines. Subsequent developments in ultrasound, including its diagnostic, therapeutic and surgical uses, all derive from Langevin’s pioneering work during WWI. Several publications and events are being planned during 2022 to mark his anniversary.
(Image credit Adrian Thomas)
|
X-RAYS TO EXILE: ARTHUR SCHÜLLER |
This 30-
Schüller was born in 1874 and the arc of his life mirrored the rise and decline of Austria from 1870 till 1955. The Schüller family origins lie in Bucovice and Brunn but his early medical career was spent in Berlin and at the AKH in Vienna.
In 1906 he married Margarete Stiassni, daughter of a wealthy Brunn industrialist. In spite of severe financial constraints on the Medical School after World War I , Arthur was closely involved in the successful graduate courses for foreign doctors who came to learn from those who had been leading figures in establishing Vienna’s pre-
As a Jew he was expelled from the University in 1938. His search for a home elsewhere involved fellow scholars in the USA, UK and Australia . After a spell in Oxford he settled in Australia with eventually at post at St Vincent’s Hospital in Melbourne.
The Schüllers’ two sons had died in Nazi camps and this appears to have provoked Arthur's later decline into withdrawal and depression. He and Margarete lived in Heidelberg, a suburb of Melbourne, until his death in 1957.
His contribution to medical science -
The link to the video is https://youtu.be/YhRLobn-
- Details
- Hits: 109075
... DEDICATED TO THE HISTORY OF RADIOLOGY IN ALL ITS FORMS...
| PAUL LANGEVIN: Physicist, Humanist, Internationalist |
A Lecture by Professor Francis Duck at the Bath Royal Literary and Scientific Institution in February 2026. Click here to watch
| THE JOHN CLIFTON ESSAY PRIZE 2026 |
About the prize
The British Society for the History of Radiology is pleased to launch the John Clifton Essay Prize for 2026, promoting research and insight into the history of radiological sciences(including medical imaging, radiotherapy and nuclear medicine).
We are keen to receive essays that explore all aspects of radiology history including scientific discovery and technological development; biographical accounts; societal impact and cultural dimensions. Essays which explore less well-known events / figures, or which demonstrate the relevance of historical events to current and future practice are encouraged.
Topics may include diagnostic imaging, interventional techniques, radiotherapy and may seek to highlight the work of radiologists, radiographers, physicists and engineers, or may explore imaging and therapeutic techniques from the patient’s perspective. Whilst entries are open to all, we particularly welcome participation from healthcare professionals in training and from undergraduates. Essays should be based on accurate historical research,but personal insights, reflections and perspectives can be included.
The prize is named in honour of Professor John Clifton (1930-2023), renowned medical physicist and member of BSHR over many years.
Competition details
Closing date: Friday 23 th October 2026
Word limit: 5000 (excluding references)
Essays should be submitted in Word, using Times New Roman Font (size 12).
Please omit the author’s name from the Word document.
Essays should be fully referenced. If images are included, it should be possible to determine
the copyright status to facilitate potential publication.
Entries must not have been previously published elsewhere.
Use of AI chatbot software or equivalent is prohibited.
Entries will be judged by members of the BSHR Council.
Entries should be sent to: This email address is being protected from spambots. You need JavaScript enabled to view it.
Prizes
First prize of £250 (and publication in Invisible Light / BSHR website)
Additional prizes may be awarded at the judges’ discretion.
Winners will also receive a year’s membership of BSHR.
All entries will be considered for publication in Invisible Light and on the BSHR website.
Winners will be announced at the BSHR Online lecture, 10 th November 2025 (further details
will be made available at bshr.org.uk)
THE BSHR ANNUAL LECTURE 2 FEBRUARY 2026
A personal History of Radiology from Röntgen to the Modern
Digital Era & AI – What can we learn from the pioneers?
by Dr Arpan K Banerjee, MBBS( LOND)FRCP FRCR FBIR, Chair ISHRAD
(International Soc History of Radiology)
Dr Banerjee has been researching and writing about radiology history for over 30 years and has published over a hundred papers and essays and several books on aspects of radiology and medical history. He is the author of ‘Radiology of AIDS’(1993), Radiology Made Easy (1999, 2006) and co author of the book ‘Classic papers in Modern Diagnostic Radiology’ (Springer 2004) and ‘The History of Radiology’ (OUP 2013). His latest project was co- editing and contributing to the book ‘Pioneers in Radiology Worldwide at the time of Wilhelm Rontgen’ published in Paris in 2024.
In this talk he will review the lives and contributions of the early radiology pioneers from Rontgen, Madame Curie and others and also cover the development of early ultrasound, CT, MRI and interventional radiology and AI. The talk will provide a historical overview of some of the key developments in radiology throughout the 20th century and the pioneers involved in these developments and will also remind us what the lives of these pioneers can teach us in our current era.
Watch the lecture: follow this link
ISHRAD
The report on the 14th ISHRAD symposium held in Gothenburg on 11 October 2025 can be found here:
https://ishrad.org/report-of-14th-symposium-of-ishrad-11-oct-2025-gothenburg-sweden
ONLINE LECTURE -- PROF IWAN MORUS on NIKOLA TESLA 6 NOVEMBER 2025
watch the online video here
| THE JOHN CLIFTON ESSAY PRIZE 2025 -WINNERS |
The Winner of the Prize this year is Katharine Thomson for her essay The First Thyroid Radionuclide Therapy
Patient? A Mystery in Time and Music. This essay will appear in Invisible Light 57.
There were awards for two Runners Ups:
Edmund Joseph: From electrotherapist to radiologist– Dawson Turner and early radiology and
Navdeep Ranar: The Body That Remains: Radiology in the Wreckage of the Atomic Age
Congratulations to all those who entered
| Other items on this page : |
Annual Lecture video |
Pioneers in Radiology Worldwide |
Past lecture videos |

A Personal History of Imaging in Radiotherapy
Prof Marcel van Herk
Click for here for the video of the 2025 Annual Lecture
| PIONEERS IN RADIOLOGY WORLDWIDE |
Some members of BSHR have contributed to a new book published and co- edited by ISHRAD (Int Soc Hist Radiology) with the SFR (French Society of Radiology). It contains 195 biographies of early radiology pioneers from 38 countries and is illustrated in colour. 250 pages.
The book 'Pioneers in Radiology Worldwide at the time of Rontgen' can be purchased from websites below.
https://eboutique.radiologie.f
https://www.livres-medicaux.c
| OTHER FEATURES |
OnLine Lecture 2024
CT: Past, Present and Future
Dr Cynthia McCollough's talk is available here
Annual Lecture 2024
Signs and Symbols: Heraldry from Roentgen to The Present Day
Stephen Keevil
OnLine Lecture 2023
The Mummy Returns
Dr Ash Chakraborty
.
- Details
- Written by Super User
- Category: Uncategorised
- Hits: 37974
A SHORT HISTORY OF RADIOLOGICAL PROTECTION
Geoff Meggitt
The origins of x-rays and radioactivity are linked: Roentgen discovered x-rays in 1895 and Becquerel stumbled upon radioactivity the following year while investigating Rontgen’s discovery. In different ways they would transform diagnostic and therapeutic medicine. However both of them brought a risk that would remain an enigma for the best part of a century (at least). That of radiation.
Roentgen revealed his discovery in the very last days of 1895 and within a few weeks radiographs had been taken around the world. Within a year there were 50 books and pamphlets on x-rays and nearly 1000 papers were published, tubes had been improved by the addition of anodes, the fluoroscope had been invented and widely used and General Electric had produced a catalogue of ready-made x-ray equipment. Soon enough, hospitals around the world were setting up departments for both diagnostic and therapeutic use of the new technology.
In the first year there were already hints of future problems. Several workers experienced effects that looked like sunburn with loss of skin and hair from affected regions. At first people blamed the high voltage power supplies and the ozone they created, the processing chemicals and almost anything but the magical rays themselves. However by September 1896 the great Lord Lister, could speak of the “aggravated sunburn” and speculate that “ a transmission of the rays through the human body may be not altogether a matter of indifference to internal organs…”
Within just a few years it became clear that prolonged exposure to the rays could have devastating consequences: sunburn turned into painful sores and warts, necrosis and a variety of cancers. The pain was “as if bones were being gnawed away by rats” someone said. Fingers were amputated, then arms. Pioneers began to die.
The warnings were heeded by some who shielded the tubes with lead and abandoned the common practice of putting their hands between the tube and a fluoroscope to check that things were working properly. By about 1910 it was fairly widely recognised that there was a problem that had to be addressed but another decade passed before there was real consensus and general action. The early protection measures were very practical: shield the tube, wear protective equipment, limit exposure by making adjustments from a protected place, limit working hours and encourage staff to spend time outdoors when they could.
A principle emerged: the deadly effects were a direct result of the traumatic tissue damage so if there was no tissue damage there would be no deadly effects. It was therefore thought that, if the dose was well below one which would result in erythema, there would be no long- term effects. This was the “tolerance dose”. In the mid-1920s a popular suggestion for a tolerance dose was about 10% of an erythema dose a year. When expressed in roentgens (r)in the early 1930s, this became 0.2 r per day and fairly quickly this was reduced to 0.1r per day. This value was the one widely used right up to the end of the 1940s.
However by then questions had begun to be asked about the principle itself based on some discoveries in genetics.
Gregor Mendel had established the theoretical existence of the genes in the 1860s with his famous experiments with peas (although the work was forgotten until the beginning of the 20th century). He had no idea where the genes were. However by the time science had rediscovered his work it was fairly clear that the nucleus of the cell played a key role in inheritance. By 1903 it was plausible that Mendel’s genes were located on the chromosomes and by 1916 that was a widely-shared view. This was largely due to the work of TH Morgan and his proteges at Columbia University in New York with the fruit fly Drosophila melanogaster. This minute creature with its modest maintenance requirements and rapid and productive sexual cycle meant that experiments like Mendel’s could be repeated in fraction of the time in a room of fly-filled phials loaded with bananas to sustain the creature. Morgan and his men tracked natural mutations ( first was a white variant of the normal red eye) and, in a long and clever series of experiments, they were able to map the mutated genes responsible onto the fly’s chromosomes the genes became real.
Hermann Muller, one of Morgan’s students, had a particular interest in how the natural mutations arose and developed an elegant technique to measure the rate at which they occurred. His first results showed a temperature dependence so, knowing that chromosomes were visibly damaged by radiation, he set about seeing how the mutation rate was affected by it. He didn’t have to wait long to find an answer: one of his first experiments in 1926 showed that an x-ray radiation dose of 1000r of x-rays to a fly’’s sperm increased the mutation rate 1000-fold.
The artificial mutations behaved just like the natural ones and, disturbingly, their creation rate increased linearly with radiation dose – without any threshold. Muller was a life-long eugenicist (although by most standards a fairly gentle one) and quickly realised the possible implications of this for the human gene pool. He spent the rest of his turbulent life campaigning for recognition of the threat.
The 1940s brought a new and awesome radiological threat with the development of the atom bomb and the terrible carnage it wrought in Japan. People soon realised that, while this had been far away, bombs were being exploded in America itself – as well as the South Pacific and Australia – in atomic tests aimed at creating even more powerful and terrifying weapons. These tests produced fallout (by now everyone knew about fallout) which swept around the world and this inevitably led to radiation exposure and this led, there being no threshold, to damage to the human gene pool.
The threat to mankind’s genes seemed ever greater. Scientists had models to enable them to make assessment of doses to the gonads and this for a while became the dominant parameter in radiation protection – largely because it was agreed that there was no threshold. Public concern about the long-term genetic effects of atomic tests was a reason why they were banned – although, more cynically, there was a sense in which the developers had gathered all the data they needed.
The threshold principle for somatic effects (those that occurred in the exposed individual) held sway through most of the 1940s but it began to be questioned – largely because it was so at variance with the established no-threshold nature of the genetic ones. So it was one of the issues in people’s minds when the Atomic Bomb Casualty Commission was set up in 1947 to study the survivors of Hiroshima and Nagasaki.
Two results of the early studies rather surprised workers: no genuine genetic effects could be found (they never were) but there was a dramatic increase in leukaemia cases and the incidence of these increased the closer you got to ground zero.
The leukaemia occurrence continued to grow but peaked in the early 1950s and then slowly declined reaching background levels in Nagasaki in about 1980.The story with solid cancers was rather different and more alarming. They were slower to appear but the incidence then stayed at a high level for much longer.
The implications of the data could not be fully realised until there were reliable estimates of the doses received by the survivors. The first of these came in 1965 and these were revised in 1986 and then again, but only slightly, in 2004.
The relationship between cancer effects and doses implied by the Japanese casualty data was regularly reviewed by the UN Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). While risk estimates were modified somewhat over the years there has never been any generally-accepted evidence to support a dose threshold for cancer induction – aligning the somatic and genetic effects. In its milestone report of 1977 (ICRP 26), when the International Commission on Radiological Protection first took full account of the available Japanese data, they opted for a no-threshold proportional relationship for both. By then it was pretty clear that the genetic effects were not the dominant effects in most circumstances, it was cancers that were.
ICRP 26 generated a protection scheme based on avoiding radiation exposures altogether unless there was a clear benefit from the activity and then optimising the exposure by increasing the protection until the cost of increasing it further was disproportionate to the dose savings. This was the As Low as Reasonably Achievable principle.
There were many technical follow-ups to the document that clarified, for example, how the risks from exposure of particular organs could be taken into account (something that was important for internal dosimetry). Applications in many fields – including medicine – have been considered in detail in ICRP reports. These reflect changes in technologies such as dosimetry techniques and new data on risks. However, the core precautionary principles have hardly changed over the subsequent four decades.
18 July 2021
This article first appeared in the Royal College of Radiologists Newsletter.
--------------------------------------------------------------------------------------
Geoff is Honorary Secretary and a Trustee of the British Society for the History of Radiology. Most of his career was spent with the United Kingdom Atomic Energy Authority and its descendants working on radiological protection. He was editor of the Journal of Radiological Protection for five years in the 1990s. Since retirement he has written two books on radiological themes: Taming the Rays (a history of radiological protection) and Genes, Flies, Bombs and a Better Life (a biography of Hermann Muller).
- You are here:
-
Home

-
Technology
- Uncategorised